Humana 2003 Annual Report Download - page 35
Download and view the complete annual report
Please find page 35 of the 2003 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
 25
25 -
 26
26 -
 27
27 -
 28
28 -
 29
29 -
 30
30 -
 31
31 -
 32
32 -
 33
33 -
 34
34 -
 35
35 -
 36
36 -
 37
37 -
 38
38 -
 39
39 -
 40
40 -
 41
41 -
 42
42 -
 43
43 -
 44
44 -
 45
45 -
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
 |
 |

The completion factor method is used for the months of incurred claims prior to the most recent three
months because the historical percentage of claims processed for those months is at a level sufficient to produce a
consistently reliable result. Conversely, for the most recent three months of incurred claims, the volume of claims
processed historically is not at a level sufficient to produce a reliable result, which therefore requires us to
examine historical trend patterns as the primary method of evaluation.
Medical cost trends potentially are more volatile than other segments of the economy. The drivers of
medical cost trends include increases in the utilization of hospital and physician services, prescription drugs, and
new medical technologies, as well as the inflationary effect on the cost per unit of each of these expense
components. Other external factors such as government-mandated benefits or other regulatory changes,
catastrophes, and epidemics also may impact medical cost trends. Additionally, as we realign our commercial
strategy, we continue to reduce the level of traditional utilization management functions such as pre-
authorization of services, monitoring of inpatient admissions, and requirements for physician referrals. Other
internal factors such as system conversions and claims processing interruptions also may impact our ability to
accurately predict estimates of historical completion factors or medical cost trends. All of these factors are
considered in estimating IBNR and in estimating the per member per month claims trend for purposes of
determining the reserve for the most recent three months. Each of these factors requires significant judgment by
management.
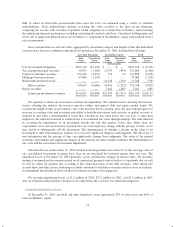
The completion and claims per member per month trend factors are the most significant factors impacting
the IBNR estimate. The following table illustrates the sensitivity of these factors and the estimated potential
impact on our operating results caused by changes in these factors based on December 31, 2003 data:
Completion Factor (a): Claims Trend Factor (b):
(Decrease)
Increase
in Factor
Increase
(Decrease) in
Medical and
Other Expenses
Payable
(Decrease)
Increase
in Factor
Increase
(Decrease) in
Medical and
Other Expenses
Payable
(dollars in thousands)
(3%) $ 136,000 (3%) $(59,000)
(2%) $ 88,000 (2%) $(41,000)
(1%) $ 43,000 (1%) $(22,000)
1% $ (40,000) 1% $ 14,000
2% $ (79,000) 2% $ 33,000
3% $(116,000) 3% $ 51,000
(a) Reflects estimated potential changes in medical and other expenses payable caused by changes in
completion factors for incurred months prior to the most recent three months.
(b) Reflects estimated potential changes in medical and other expenses payable caused by changes in
annualized claims trend used for the estimation of per member per month incurred claims for the most
recent three months.
Most medical claims are paid within a few months of the member receiving service from a physician or
other health care provider. As a result, these liabilities generally are described as having a “short-tail”, which
causes less than 2% of our medical and other expenses payable as of the end of any given period to be
outstanding for more than 12 months. As such, we expect that substantially all of the 2003 estimate of medical
and other expenses payable will be known and paid during 2004.
Our reserving practice is to consistently recognize the actuarial best point estimate within a level of
confidence required by actuarial standards. Actuarial standards of practice generally require a level of confidence
such that the liabilities established for IBNR have a greater probability of being adequate versus being
insufficient, or such that the liabilities established for IBNR are sufficient to cover obligations under an
assumption of moderately adverse conditions. Adverse conditions are situations in which the actual claims are
27