Humana 2002 Annual Report Download - page 31
Download and view the complete annual report
Please find page 31 of the 2002 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
 21
21 -
 22
22 -
 23
23 -
 24
24 -
 25
25 -
 26
26 -
 27
27 -
 28
28 -
 29
29 -
 30
30 -
 31
31 -
 32
32 -
 33
33 -
 34
34 -
 35
35 -
 36
36 -
 37
37 -
 38
38 -
 39
39 -
 40
40 -
 41
41 -
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
 |
 |
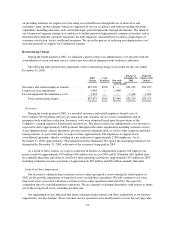
of certain long-lived assets, primarily buildings used in these operations. Accordingly, we adjusted the carrying
value of these long-lived assets to their estimated fair value resulting in a non-cash impairment charge of
$2.4 million ($1.5 million after tax). Estimated fair value was based on an independent third party appraisal of
the buildings.
By the end of the first quarter of 2003, we expect the estimated future undiscounted cash flow attributable to
our business supported by our Jacksonville, Florida customer service operations will be insufficient to recover
the carrying value of additional long-lived assets, primarily a building used in our Florida operations.
Accordingly, we expect to record a non-cash impairment charge of approximately $17.2 million ($10.5 million
after tax) during the first quarter of 2003. Additionally, we expect to record a non-cash impairment charge of
approximately $13.5 million during the first quarter of 2003 ($8.3 million after tax) related to accelerated
depreciation of software we will cease using with these operations.
As a result of these actions, we expect a reduction in historical depreciation and rent expense will improve
our pretax results by approximately $5 million ($3 million after tax) in 2003 and $6 million ($4 million after tax)
annually thereafter. The impact on operating cash flows is not expected to be material.
Critical Accounting Policies and Estimates
The discussion and analysis of our financial condition and results of operations is based upon our
consolidated financial statements and accompanying notes, which have been prepared in accordance with
accounting principles generally accepted in the United States of America. The preparation of these financial
statements and accompanying notes requires us to make estimates and assumptions that affect the amounts
reported in the financial statements and accompanying notes. We continuously evaluate our estimates and those
critical accounting policies related primarily to medical cost and revenue recognition as well as accounting for
impairments related to our investment securities, goodwill, and long-lived assets. These estimates are based on
knowledge of current events and anticipated future events, and accordingly, actual results may ultimately differ
from those estimates. We believe the following critical accounting policies involve the most significant
judgments and estimates used in the preparation of our consolidated financial statements.
Medical Cost Recognition
Medical costs include claim payments, capitation payments, allocations of certain centralized expenses and
various other costs incurred to provide health insurance coverage to members, as well as estimates of future
payments to hospitals and others for medical care provided prior to the balance sheet date. Capitation payments
represent monthly contractual fees disbursed to primary care physicians and other providers who are responsible
for providing medical care to members. We estimate the costs of our future medical claims and other medical
expense payments using actuarial methods and assumptions based upon claim payment patterns, medical cost
inflation, historical developments such as claim inventory levels and claim receipt patterns, and other relevant
factors, and record medical claims reserves for future payments. We continually review estimates of future
payments relating to medical claims costs for services incurred in the current and prior periods and make
necessary adjustments to our reserves.
Medical cost inflation, among other items, may significantly impact our estimate of medical costs. Medical
cost inflationary trends today are substantially higher than other segments of the economy. In the early 1990’s
employer-driven migration to HMO enrollment was popular and resulted in several years of very low medical
cost trends. Today, there are very few economic forces existing to mitigate increases in the utilization of hospital
and physician services, prescription drugs and new medical technologies, and the inflationary trend on the cost
per unit for each of these expense components. Additionally, as we are realigning our operating model around
our commercial strategy, we continue to reduce the level of traditional utilization management functions such as
pre-authorization of services, monitoring of inpatient admissions and requirements for physician referrals. Other
external factors such as government mandated benefits or other regulatory changes, catastrophes and epidemics
may also impact cost trends.
25