Humana 2008 Annual Report Download - page 16
Download and view the complete annual report
Please find page 16 of the 2008 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
 6
6 -
 7
7 -
 8
8 -
 9
9 -
 10
10 -
 11
11 -
 12
12 -
 13
13 -
 14
14 -
 15
15 -
 16
16 -
 17
17 -
 18
18 -
 19
19 -
 20
20 -
 21
21 -
 22
22 -
 23
23 -
 24
24 -
 25
25 -
 26
26 -
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
-
127
-
128
-
129
-
130
-
131
-
132
-
133
-
134
-
135
-
136
 |
 |
indicators, or risk scores, to improve the adequacy of payment. The risk-adjustment model, which CMS
implemented pursuant to the Balanced Budget Act of 1997 (BBA) and the Benefits and Improvement Protection
Act of 2000 (BIPA), generally pays more for members with predictably higher costs and uses principal hospital
inpatient diagnoses as well as diagnosis data from ambulatory treatment settings (hospital outpatient department
and physician visits). CMS transitioned to this risk-based reimbursement model while the old reimbursement
model based on demographic data including gender, age, and disability status was phased out. The phase-in of
risk adjusted payment was completed in 2007. Under the risk-adjustment methodology, all health benefit
organizations must capture, collect, and submit the necessary diagnosis code information to CMS within
prescribed deadlines.
Commensurate with the phase-in of the risk-adjustment methodology, payments to Medicare Advantage
plans were increased by a “budget neutrality” factor. The budget neutrality factor was implemented to prevent
overall health plan payments from being reduced during the transition from the previous reimbursement model,
based upon average original Medicare fee-for-service spending, to the risk-adjustment payment model. The
budget neutrality adjustment began phasing out in 2007 and will be fully eliminated by 2011.
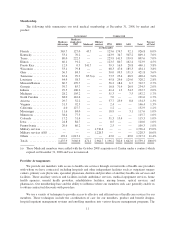
At December 31, 2008, we provided health insurance coverage under CMS contracts to approximately
1,435,900 MA-PD members for which we received premium revenues of approximately $13.8 billion, or 48.3%
of our total premiums and ASO fees for the year ended December 31, 2008. Under our Medicare Advantage
contracts with CMS in Florida, we provided health insurance coverage to approximately 365,700 members.
These contracts accounted for premium revenues of approximately $4.5 billion, which represented approximately
32.6% of our Medicare Advantage premium revenues, or 15.7% of our total premiums and ASO fees for the year
ended December 31, 2008.
Our HMO, PFFS, and PPO products covered under Medicare Advantage contracts with CMS are renewed
generally for a one-year term each December 31 unless CMS notifies Humana of its decision not to renew by
August 1 of the year in which the contract would end, or Humana notifies CMS of its decision not to renew by
the first Monday in June of the year in which the contract would end. All material contracts between Humana and
CMS relating to our Medicare Advantage business have been renewed for 2009.
Medicare Stand-Alone Prescription Drug Products
On January 1, 2006, we began offering stand-alone prescription drug plans, or PDPs, under Medicare
Part D. Generally, Medicare-eligible individuals enroll in one of our three plan choices between November 15
and December 31 for coverage that begins January 1. Our stand-alone PDP offerings consist of plans offering
basic coverage with benefits mandated by Congress, as well as plans providing enhanced coverage with varying
degrees of out-of-pocket costs for premiums, deductibles and co-insurance. Our revenues from CMS and the
beneficiary are determined from our bids submitted annually to CMS. These revenues also reflect the health
status of the beneficiary and risk sharing provisions as more fully described beginning on page 58. Our stand-
alone PDP contracts with CMS are renewed generally for a one-year term each December 31 unless CMS
notifies Humana of its decision not to renew by August 1 of the year in which the contract would end, or Humana
notifies CMS of its decision not to renew by the first Monday in June of the year in which the contract would
end. All material contracts between Humana and CMS relating to our Medicare stand-alone PDP business have
been renewed for 2009.
Medicaid Product
Medicaid is a federal program that is state-operated to facilitate the delivery of health care services
primarily to low-income residents. Each electing state develops, through a state-specific regulatory agency, a
Medicaid managed care initiative that must be approved by CMS. CMS requires that Medicaid managed care
plans meet federal standards and cost no more than the amount that would have been spent on a comparable
fee-for-service basis. States currently either use a formal proposal process in which they review many bidders
6