Humana 2012 Annual Report Download - page 55
Download and view the complete annual report
Please find page 55 of the 2012 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
 45
45 -
 46
46 -
 47
47 -
 48
48 -
 49
49 -
 50
50 -
 51
51 -
 52
52 -
 53
53 -
 54
54 -
 55
55 -
 56
56 -
 57
57 -
 58
58 -
 59
59 -
 60
60 -
 61
61 -
 62
62 -
 63
63 -
 64
64 -
 65
65 -
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
-
127
-
128
-
129
-
130
-
131
-
132
-
133
-
134
-
135
-
136
-
137
-
138
-
139
-
140
-
141
-
142
-
143
-
144
-
145
-
146
-
147
-
148
-
149
-
150
-
151
-
152
-
153
-
154
-
155
-
156
-
157
-
158
-
159
-
160
-
161
-
162
-
163
-
164
 |
 |
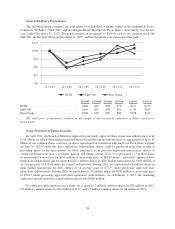
• Year-over-year comparisons within Other Businesses are impacted by the transition to the new
TRICARE South Region contract on April 1, 2012, including a change in profitability under the new
contract in connection with our bid strategy, benefits expense of approximately $46 million incurred
related to the settlement of litigation associated with our military services business during 2012, and
benefits expense of $29 million for reserve strengthening associated with our closed-block of long-term
care policies during 2012 as discussed in Note 17 to the consolidated financial statements included in
Item 8. – Financial Statements and Supplementary Data.
Health Insurance Reform
The Patient Protection and Affordable Care Act and The Health Care and Education Reconciliation Act of
2010 (which we collectively refer to as the Health Insurance Reform Legislation) enacted significant reforms to
various aspects of the U.S. health insurance industry. While regulations and interpretive guidance on some
provisions of the Health Insurance Reform Legislation have been issued to date by the Department of Health and
Human Services, or HHS, the Department of Labor, the Treasury Department, and the National Association of
Insurance Commissioners, there are many provisions of the legislation that will require additional guidance and
clarification in the form of regulations and interpretations in order to fully understand the impacts of the
legislation on our overall business, which we expect to occur over the next several years.
Implementation dates of the Health Insurance Reform Legislation began in September 2010 and continue
through 2018. The following outlines certain provisions of the Health Insurance Reform Legislation:
• Many changes are already effective and have been implemented by the Company, including:
elimination of pre-existing condition limits for enrollees under age 19, elimination of certain annual
and lifetime caps on the dollar value of benefits, expansion of dependent coverage to include adult
children until age 26, a requirement to provide coverage for prescribed preventive services without cost
to members, new claim appeal requirements, and the establishment of an interim high risk program for
those unable to obtain coverage due to a pre-existing condition or health status.
• Effective January 1, 2011, minimum benefit ratios were mandated for all commercial fully-insured
medical plans in the large group (85%), small group (80%), and individual (80%) markets, with annual
rebates to policyholders if the actual benefit ratios, calculated in a manner prescribed by HHS, do not
meet these minimums. We began accruing for rebates in 2011, based on the manner prescribed by
HHS, with initial rebate payments made in July 2012. Our benefit ratios reported herein, calculated
from financial statements prepared in accordance with accounting principles generally accepted in the
United States of America, or GAAP, differ from the benefit ratios calculated as prescribed by HHS
under the Health Insurance Reform Legislation. The more noteworthy differences include the fact that
the benefit ratio calculations prescribed by HHS are calculated separately by state and legal entity;
independently for individual, small group, and large group fully-insured products; reflect actuarial
adjustments where the membership levels are not large enough to create credible size; exclude some of
our health insurance products; include taxes and fees as reductions of premium; treat changes in
reserves differently than GAAP; and classify rebate amounts as additions to incurred claims as opposed
to adjustments to premiums for GAAP reporting.
• Medicare Advantage payment benchmarks for 2011 were frozen at 2010 levels and in 2012, additional
cuts to Medicare Advantage plan payments began to take effect (with plan payment benchmarks
ultimately ranging from 95% in high-cost areas to 115% in low-cost areas of Medicare fee-for-service
rates), with changes being phased-in over two to six years, depending on the level of payment
reduction in a county. In addition, beginning in 2011 the gap in coverage for Medicare Part D
prescription drug coverage is incrementally closing.
• Beginning in 2014, the Health Insurance Reform Legislation requires: all individual and group health
plans to guarantee issuance and renew coverage without pre-existing condition exclusions or health-
status rating adjustments; the elimination of annual limits on coverage on certain plans; the
45