Humana 2012 Annual Report Download - page 89
Download and view the complete annual report
Please find page 89 of the 2012 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
 79
79 -
 80
80 -
 81
81 -
 82
82 -
 83
83 -
 84
84 -
 85
85 -
 86
86 -
 87
87 -
 88
88 -
 89
89 -
 90
90 -
 91
91 -
 92
92 -
 93
93 -
 94
94 -
 95
95 -
 96
96 -
 97
97 -
 98
98 -
 99
99 -
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
-
127
-
128
-
129
-
130
-
131
-
132
-
133
-
134
-
135
-
136
-
137
-
138
-
139
-
140
-
141
-
142
-
143
-
144
-
145
-
146
-
147
-
148
-
149
-
150
-
151
-
152
-
153
-
154
-
155
-
156
-
157
-
158
-
159
-
160
-
161
-
162
-
163
-
164
 |
 |
diagnosis code information from hospital inpatient, hospital outpatient, and physician providers to CMS within
prescribed deadlines. The CMS risk-adjustment model uses this diagnosis data to calculate the risk-adjusted
premium payment to Medicare Advantage plans. Rates paid to Medicare Advantage plans are established under
an actuarial bid model, including a process that bases our payments on a comparison of our beneficiaries’ risk
scores, derived from medical diagnoses, to those enrolled in the government’s original Medicare program. We
generally rely on providers, including certain providers in our network who are our employees, to code their
claim submissions with appropriate diagnoses, which we send to CMS as the basis for our payment received
from CMS under the actuarial risk-adjustment model. We also rely on providers to appropriately document all
medical data, including the diagnosis data submitted with claims. We estimate risk-adjustment revenues based on
medical diagnoses for our membership. The risk-adjustment model is more fully described in Item 1. – Business
under the section titled “Individual Medicare.”
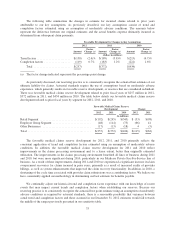
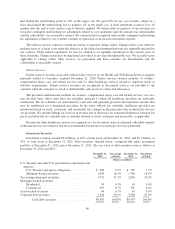
Military services
In 2012, revenues derived from our military services business represented approximately 3% of total
premiums and services revenue. Military services premiums and services revenue primarily is derived from our
TRICARE South Region contract with the Department of Defense, or DoD. On April 1, 2012, we began
delivering services under a new TRICARE South Region contract with the DoD. Under the new contract, we
provide administrative services, including offering access to our provider networks and clinical programs, claim
processing, customer service, enrollment, and other services, while the federal government retains all of the risk
of the cost of health benefits. Under the terms of the new TRICARE South Region contract, we do not record
premiums revenue or benefits expense in our consolidated statements of income related to these health care costs
and related reimbursements. Instead, we account for revenues under the new contract net of estimated health care
costs similar to an administrative services fee only agreement. The new contract includes fixed administrative
services fees and incentive fees and penalties. Administrative services fees are recognized as services are
performed.
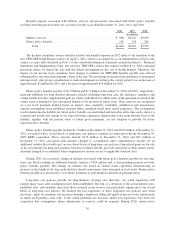
Our TRICARE members are served by both in-network and out-of-network providers in accordance with the
new contract. We pay health care costs related to these services to the providers and are subsequently reimbursed
by the DoD for such payments. We account for the payments associated with these health care costs and the
related reimbursements under deposit accounting in our consolidated balance sheets and as a financing activity
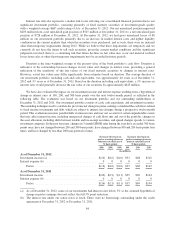
under receipts (withdrawals) from contract deposits in our consolidated statements of cash flows. For the first
nine months of the new contract, April 1, 2012 to December 31, 2012, health care cost payments were $2.1
billion, exceeding reimbursements of $2.0 billion by $56 million.
Our previous TRICARE South Region contract that expired on March 31, 2012 provided a financial interest
in the underlying health care cost; therefore, we reported revenues on a gross basis. We shared the risk with the
federal government for the cost of health benefits incurred under our previous contract, earning more revenue or
incurring additional cost based on the variance of actual health care costs from an annually negotiated target
health care cost as described below. TRICARE revenues consisted generally of (1) an insurance premium for
assuming underwriting risk for the cost of civilian health care services delivered to eligible beneficiaries;
(2) health care services provided to beneficiaries which were in turn reimbursed by the federal government; and
(3) administrative services fees related to claim processing, customer service, enrollment, and other services. We
recognized the insurance premium as revenue ratably over the period coverage was provided. Health care
services reimbursements were recognized as revenue in the period health services were provided. Administrative
services fees were recognized as revenue in the period services were performed.
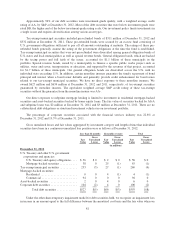
As indicated above, our previous TRICARE South Region contained provisions where we shared the risk
with the federal government for the cost of health benefits. Annually, we negotiated a target health care cost
amount, or target cost, with the federal government and determined an underwriting fee. Any variance from the
target cost was shared. We earned more revenue or incurred additional costs based on the variance of actual
health care costs versus the negotiated target cost. We received 20% for any cost underrun, subject to a ceiling
79