Humana 2006 Annual Report Download - page 82
Download and view the complete annual report
Please find page 82 of the 2006 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
 72
72 -
 73
73 -
 74
74 -
 75
75 -
 76
76 -
 77
77 -
 78
78 -
 79
79 -
 80
80 -
 81
81 -
 82
82 -
 83
83 -
 84
84 -
 85
85 -
 86
86 -
 87
87 -
 88
88 -
 89
89 -
 90
90 -
 91
91 -
 92
92 -
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
 |
 |
Humana Inc.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
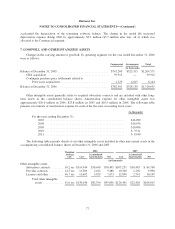
specialty. The Government segment’s three reporting units consist of Medicare, TRICARE and Medicaid.
Goodwill is assigned to the reporting unit that is expected to benefit from a specific acquisition.
SFAS 142 requires a two-step process to review goodwill for impairment. The first step is a screen for
potential impairment, and the second step measures the amount of impairment, if any. Impairment tests are
performed, at a minimum, in the fourth quarter of each year supported by our long-range business plan and
annual planning process. Impairment tests completed for 2006, 2005 and 2004 did not result in an impairment
loss.
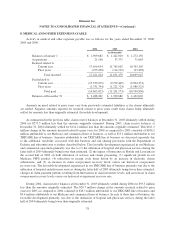
Other intangible assets primarily relate to acquired subscriber and provider contracts and are included with
other long-term assets in the consolidated balance sheets. Other intangible assets are amortized over the useful
life, based upon the pattern of future cash flows attributable to the asset. This sometimes results in an accelerated
method of amortization for subscriber contracts because the asset tends to dissipate at a more rapid rate in earlier
periods. Other than subscriber contracts, other intangible assets generally are amortized using the straight-line
method. We review other finite-lived intangible assets for impairment under our long-lived asset policy.
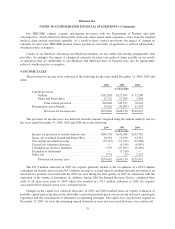
Medical and Other Expenses Payable and Medical Cost Recognition
Medical costs include claim payments, capitation payments, pharmacy costs net of rebates, allocations of
certain centralized expenses and various other costs incurred to provide health insurance coverage to members, as
well as estimates of future payments to hospitals and others for medical care provided prior to the balance sheet
date. Capitation payments represent monthly contractual fees disbursed to primary care physicians and other
providers who are responsible for providing medical care to members. Pharmacy costs represent payments for
members’ prescription drug benefits, net of rebates from drug manufacturers. Receivables for such pharmacy
rebates are included in other current assets in the consolidated balance sheets.
We estimate the costs of our medical claims and other medical expense payments using actuarial methods
and assumptions based upon claim payment patterns, medical cost inflation, historical developments such as
claim inventory levels and claim receipt patterns, and other relevant factors, and record medical claims reserves
for future payments. We continually review estimates of future payments relating to medical claims costs for
services incurred in the current and prior periods and make necessary adjustments to our reserves.
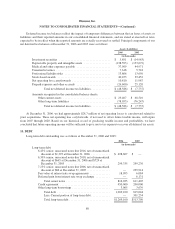
We reassess the profitability of our contracts for providing health insurance coverage to our members when
current operating results or forecasts indicate probable future losses. We establish a premium deficiency liability
in current operations to the extent that the sum of expected future medical costs, claim adjustment expenses, and
maintenance costs exceeds related future premiums under contract without consideration of investment income.
For purposes of premium deficiencies, contracts are grouped in a manner consistent with our method of
acquiring, servicing, and measuring the profitability of such contracts. Losses recognized as a premium
deficiency result in a beneficial effect in subsequent periods as operating losses under these contracts are charged
to the liability previously established. There were no premium deficiency liabilities recorded at December 31,
2006 and 2005. Because the majority of our member contracts renew annually, we do not anticipate recording a
premium deficiency liability, except when unanticipated adverse events or changes in circumstances indicate
otherwise.
For our health and life policies sold to individuals and accounted for as long-duration insurance products
under the provisions of SFAS 60, medical and other expenses payable include liabilities for future policy benefits
for which some of the premium received in the earlier years is intended to pay anticipated benefits to be incurred
in future years.
70