Humana 2009 Annual Report Download - page 71
Download and view the complete annual report
Please find page 71 of the 2009 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
 61
61 -
 62
62 -
 63
63 -
 64
64 -
 65
65 -
 66
66 -
 67
67 -
 68
68 -
 69
69 -
 70
70 -
 71
71 -
 72
72 -
 73
73 -
 74
74 -
 75
75 -
 76
76 -
 77
77 -
 78
78 -
 79
79 -
 80
80 -
 81
81 -
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
-
127
-
128
-
129
-
130
-
131
-
132
-
133
-
134
-
135
-
136
-
137
-
138
-
139
-
140
 |
 |
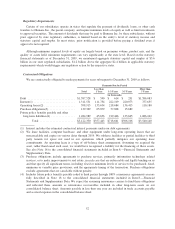
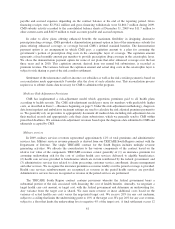
payable and accrued expenses depending on the contract balance at the end of the reporting period. Gross
financing receipts were $2,354.2 million and gross financing withdrawals were $1,860.7 million during 2009.
CMS subsidy activity recorded to the consolidated balance sheets at December 31, 2009 was $11.7 million to
other current assets and $402.9 million to trade accounts payable and accrued expenses.
In order to allow plans offering enhanced benefits the maximum flexibility in designing alternative
prescription drug coverage, CMS provided a demonstration payment option in lieu of the reinsurance subsidy for
plans offering enhanced coverage, or coverage beyond CMS’s defined standard benefits. The demonstration
payment option is an arrangement in which CMS pays a capitation amount to a plan for assuming the
government’s portion of prescription drug costs in the catastrophic layer of coverage. The capitation amount
represents a fixed monthly amount per member to provide prescription drug coverage in the catastrophic layer.
We chose the demonstration payment option for some of our plans that offer enhanced coverage over the last
three years and in 2010. This capitation amount, derived from our annual bid submissions, is recorded as
premium revenue. The variance between the capitation amount and actual drug costs in the catastrophic layer is
subject to risk sharing as part of the risk corridor settlement.
Settlement of the reinsurance and low-income cost subsidies as well as the risk corridor payment is based on
a reconciliation made approximately 9 months after the close of each calendar year. This reconciliation process
requires us to submit claims data necessary for CMS to administer the program.
Medicare Risk-Adjustment Provisions
CMS has implemented a risk-adjustment model which apportions premiums paid to all health plans
according to health severity. The CMS risk-adjustment model pays more for members with predictably higher
costs, as described in Item 1.—Business beginning on page 5. Under this risk-adjustment methodology, diagnosis
data from inpatient and ambulatory treatment settings are used to calculate the risk adjusted premium payment to
us. We generally rely on providers to appropriately document all medical data including risk-adjustment data in
their medical records and appropriately code their claim submissions, which we generally send to CMS within
prescribed deadlines. We estimate risk-adjustment revenues based upon the diagnosis data submitted to CMS and
ultimately accepted by CMS.
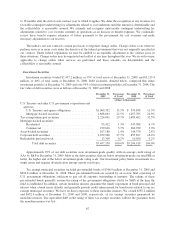
Military services
In 2009, military services revenues represented approximately 12% of total premiums and administrative
services fees. Military services revenue primarily is derived from our TRICARE South Region contract with the
Department of Defense. The single TRICARE contract for the South Region includes multiple revenue
generating activities. We allocate the consideration to the various components of the contract based on the
relative fair value of the components. TRICARE revenues consist generally of (1) an insurance premium for
assuming underwriting risk for the cost of civilian health care services delivered to eligible beneficiaries;
(2) health care services provided to beneficiaries which are in turn reimbursed by the federal government; and
(3) administrative services fees related to claim processing, customer service, enrollment, disease management
and other services. We recognize the insurance premium as revenue ratably over the period coverage is provided.
Health care services reimbursements are recognized as revenue in the period health services are provided.
Administrative services fees are recognized as revenue in the period services are performed.
The TRICARE South Region contract contains provisions whereby the federal government bears a
substantial portion of the risk associated with financing the cost of health benefits. Annually, we negotiate a
target health care cost amount, or target cost, with the federal government and determine an underwriting fee.
Any variance from the target cost is shared. We earn more revenue or incur additional costs based on the
variance of actual health care costs versus the negotiated target cost. We receive 20% for any cost underrun,
subject to a ceiling that limits the underwriting profit to 10% of the target cost. We pay 20% for any cost overrun,
subject to a floor that limits the underwriting loss to negative 4% of the target cost. A final settlement occurs 12
61