Humana 2004 Annual Report Download - page 53
Download and view the complete annual report
Please find page 53 of the 2004 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
 43
43 -
 44
44 -
 45
45 -
 46
46 -
 47
47 -
 48
48 -
 49
49 -
 50
50 -
 51
51 -
 52
52 -
 53
53 -
 54
54 -
 55
55 -
 56
56 -
 57
57 -
 58
58 -
 59
59 -
 60
60 -
 61
61 -
 62
62 -
 63
63 -
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
 |
 |
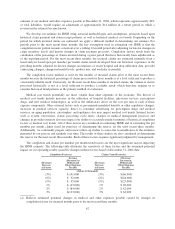
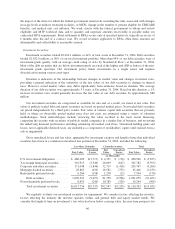
(b) Reflects estimated potential changes in medical and other expenses payable caused by changes in
annualized claims trend used for the estimation of per member per month incurred claims for the most
recent three months.
Most medical claims are paid within a few months of the member receiving service from a physician or
other health care provider. As a result, these liabilities generally are described as having a “short-tail”, which
causes less than 2% of our medical and other expenses payable as of the end of any given period to be
outstanding for more than 12 months. As such, we expect that substantially all of the 2004 estimate of medical
and other expenses payable will be known and paid during 2005.
Our reserving practice is to consistently recognize the actuarial best point estimate within a level of
confidence required by actuarial standards. Actuarial standards of practice generally require a level of confidence
such that the liabilities established for IBNR have a greater probability of being adequate versus being
insufficient, or such that the liabilities established for IBNR are sufficient to cover obligations under an
assumption of moderately adverse conditions. Adverse conditions are situations in which the actual claims are
expected to be higher than the otherwise estimated value of such claims at the time of the estimate. Therefore, in
many situations, the claim amounts ultimately settled will be less than the estimate that satisfies the actuarial
standards of practice.
IBNR established in connection with our TRICARE contracts is typically more difficult to estimate than for
our other operations, because there are more variables that impact the estimate. These variables include continual
changes in the number of eligible beneficiaries, changes in the utilization of military treatment facilities and
changes in levels of benefits versus the original contract provisions. Many of these variables are impacted
significantly by an increase or decrease in military activity involving the United States armed forces.
Additionally, we transitioned to the new TRICARE South Region contract during the latter half of 2004.
Accordingly, our historical claims experience and familiarity with claim payment patterns for this block of
business is not as mature as our other lines of business. We have considered all of these factors in establishing
our IBNR estimate. Each of these factors required significant judgment by management.
As more fully described on page 45, our TRICARE contract contains risk-sharing provisions with the
Department of Defense and with subcontractors, which effectively limit profits and losses when actual claim
experience varies from the targeted medical claim amount negotiated in our annual bid. As a result of these
contract provisions, the impact of changes in estimates for prior year TRICARE medical claims payable on our
results of operations is reduced substantially, whether positive or negative.
As more fully described on pages 10 and 11, we have a substantial percentage of our Medicare and
Medicaid membership under risk-sharing arrangements with providers. Accordingly, the impact of changes in
estimates for prior year medical claims payable on our results from operations that are attributable to our
Medicare and Medicaid lines of business may also be significantly reduced, whether positive or negative.
43