Humana 2004 Annual Report Download - page 55
Download and view the complete annual report
Please find page 55 of the 2004 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
 45
45 -
 46
46 -
 47
47 -
 48
48 -
 49
49 -
 50
50 -
 51
51 -
 52
52 -
 53
53 -
 54
54 -
 55
55 -
 56
56 -
 57
57 -
 58
58 -
 59
59 -
 60
60 -
 61
61 -
 62
62 -
 63
63 -
 64
64 -
 65
65 -
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
 |
 |
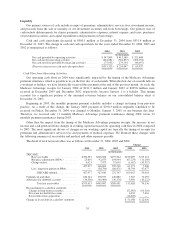
such as age, working status, or specific health issues of the member. Changes in revenues from CMS for our
Medicare Advantage products resulting from the periodic changes in risk adjustment scores for our membership
are recognized when the amounts become determinable and the collectibility is reasonably assured.
Premium revenues and ASO fees are estimated by multiplying the membership covered under the various
contracts by the contractual rates. In addition, we adjust revenues for estimated changes in an employer’s
enrollment and customers that ultimately may fail to pay. Enrollment changes not yet reported by an employer
group, an individual, or the government, also known as retroactive membership adjustments, are estimated based
on historical trends. We monitor the collectibility of specific accounts, the aging of receivables, as well as
prevailing and anticipated economic conditions, and reflect any required adjustments in the current period’s
revenue.
We bill and collect premium and ASO fee remittances from employer groups, the federal and state
governments, and individual Medicare Advantage members monthly. Premium and ASO fee receivables are
presented net of allowances for estimated uncollectible accounts and retroactive membership adjustments.
Premiums and ASO fees received prior to the period members are entitled to receive services are recorded as
unearned revenues.
TRICARE Contract
In 2004, TRICARE revenues represented 17% of total premiums and administrative services fees. The
single TRICARE contract for the South Region includes multiple revenue generating activities and as such was
evaluated under Emerging Issues Task Force (EITF) Issue No. 00-21, Accounting for Revenue Arrangements
with Multiple Deliverables. We allocate the consideration to the various components based on the relative fair
values of the components. TRICARE revenues consist generally of (1) an insurance premium for assuming
underwriting risk for the cost of civilian healthcare services delivered to eligible beneficiaries; (2) healthcare
services provided to beneficiaries which are in turn reimbursed by the federal government; and, (3)
administrative service fees related to claim processing, customer service, enrollment, disease management and
other services. We recognize the insurance premium as revenue ratably over the period coverage is provided.
Health care services reimbursements are recognized as revenue in the period health care services are provided.
Administrative service fees are recognized as revenue in the period services are performed.
The TRICARE contract contains provisions whereby the federal government bears a substantial portion of
the risk associated with financing the cost of health benefits. Annually, we negotiate a target healthcare cost
amount, or target cost, with the federal government and determine an underwriting fee. Any variance from the
target cost is shared. We earn more revenue or incur additional costs based on the variance in actual health care
costs versus the negotiated target cost. We receive 20% for any cost underrun, subject to a ceiling that limits the
underwriting profit to 10% of the target cost. We pay 20% for any cost overrun, subject to a floor that limits the
underwriting loss to negative 4% of the target cost. A final settlement occurs 12 to 18 months after the end of
each contract year to which it applies. We defer the recognition of any revenues for favorable contingent
underwriting fee adjustments related to cost underruns until the amount is determinable and the collectibility is
reasonably assured. We estimate and recognize unfavorable contingent underwriting fee adjustments related to
cost overruns currently in operations as an increase in medical expenses.
The TRICARE contract contains provisions to negotiate change orders. Change orders occur when we
perform services or incur costs under the directive of the federal government that were not originally specified in
our contract. Under federal regulations we may be entitled to an equitable adjustment to the contract price in
these situations. Change orders may be negotiated and settled at any time throughout the year. We record revenue
applicable to change orders when services are performed and these amounts are determinable and collectibility is
reasonably assured.
Our former TRICARE contracts for Regions 3 and 4 and Regions 2 and 5, which expired during 2004,
contained provisions for not only change orders but for bid price adjustments, or BPAs as well. There are no
provisions for BPAs in our current TRICARE contract. BPAs were utilized to retroactively adjust revenues for
45