Humana 2013 Annual Report Download - page 25
Download and view the complete annual report
Please find page 25 of the 2013 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
 15
15 -
 16
16 -
 17
17 -
 18
18 -
 19
19 -
 20
20 -
 21
21 -
 22
22 -
 23
23 -
 24
24 -
 25
25 -
 26
26 -
 27
27 -
 28
28 -
 29
29 -
 30
30 -
 31
31 -
 32
32 -
 33
33 -
 34
34 -
 35
35 -
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
-
127
-
128
-
129
-
130
-
131
-
132
-
133
-
134
-
135
-
136
-
137
-
138
-
139
-
140
-
141
-
142
-
143
-
144
-
145
-
146
-
147
-
148
-
149
-
150
-
151
-
152
-
153
-
154
-
155
-
156
-
157
-
158
-
159
-
160
-
161
-
162
-
163
-
164
-
165
-
166
-
167
-
168
 |
 |
We typically contract with hospitals on either (1) a per diem rate, which is an all-inclusive rate per day, (2) a
case rate or diagnosis-related groups (DRG), which is an all-inclusive rate per admission, or (3) a discounted
charge for inpatient hospital services. Outpatient hospital services generally are contracted at a flat rate by type of
service, ambulatory payment classifications, or APCs, or at a discounted charge. APCs are similar to flat rates
except multiple services and procedures may be aggregated into one fixed payment. These contracts are often
multi-year agreements, with rates that are adjusted for inflation annually based on the consumer price index,
other nationally recognized inflation indexes, or specific negotiations with the provider. Outpatient surgery
centers and other ancillary providers typically are contracted at flat rates per service provided or are reimbursed
based upon a nationally recognized fee schedule such as the Medicare allowable fee schedule.
Our contracts with physicians typically are renewed automatically each year, unless either party gives
written notice, generally ranging from 90 to 120 days, to the other party of its intent to terminate the
arrangement. Most of the physicians in our PPO networks and some of our physicians in our HMO networks are
reimbursed based upon a fixed fee schedule, which typically provides for reimbursement based upon a
percentage of the standard Medicare allowable fee schedule.
The terms of our contracts with hospitals and physicians may also vary between Medicare and commercial
business. A significant portion of our Medicare network contracts, including those with both hospitals and
physicians, are tied to Medicare reimbursement levels and methodologies.
The Budget Control Act of 2011, enacted on August 2, 2011, increased the United States debt ceiling
conditioned on deficit reductions to be achieved over the next ten years. The Budget Control Act of 2011 also
established a twelve-member joint committee of Congress known as the Joint Select Committee on Deficit
Reduction to propose legislation to reduce the United States federal deficit by $1.5 trillion for fiscal years 2012-
2021. The failure of the Joint Select Committee on Deficit Reduction to achieve a targeted deficit reduction by
December 23, 2011 triggered an automatic reduction, including aggregate reductions to Medicare payments to
providers of up to 2 percent per fiscal year. These reductions took effect on April 1, 2013, and the Bipartisan
Budget Act of 2013, enacted on December 26, 2013, extended the reductions for two years. We expect a
corresponding substantial reduction in our obligations to providers. Due to the uncertainty around the application
of any such reductions, there can be no assurances that we can completely offset any reductions to the Medicare
healthcare programs applied by the Budget Control Act of 2011. See “Legal Proceedings and Certain Regulatory
Matters” in Note 15 to the consolidated financial statements included in Item 8. – Financial Statements and
Supplementary Data.
Capitation
For some of our medical membership, we share risk with providers under capitation contracts where
physicians and hospitals accept varying levels of financial risk for a defined set of membership, primarily HMO
membership. Under the typical capitation arrangement, we prepay these providers a monthly fixed-fee per
member, known as a capitation (per capita) payment, to cover all or a defined portion of the benefits provided to
the capitated member.
We believe these risk-based models represent a key element of our integrated care delivery model at the
core of our strategy. Our health plan subsidiaries may enter into these risk-based contracts with third party
providers or our owned provider subsidiaries, including Metropolitan, an MSO acquired December 21, 2012.
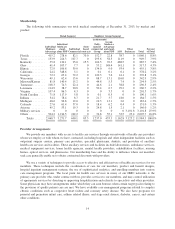
At December 31, 2013, approximately 671,000 members, or 5.6% of our medical membership, were
covered under risk-based contracts, including 561,500 individual Medicare Advantage members, or 27.1% of our
total individual Medicare Advantage membership. The termination of our Puerto Rico Medicaid contract
effective September 30, 2013 resulted in a decline in the total number of members covered under risk-based
contracts from 1,131,700 members at December 31, 2012.
15