Humana 2013 Annual Report Download - page 59
Download and view the complete annual report
Please find page 59 of the 2013 Humana annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
 49
49 -
 50
50 -
 51
51 -
 52
52 -
 53
53 -
 54
54 -
 55
55 -
 56
56 -
 57
57 -
 58
58 -
 59
59 -
 60
60 -
 61
61 -
 62
62 -
 63
63 -
 64
64 -
 65
65 -
 66
66 -
 67
67 -
 68
68 -
 69
69 -
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
-
127
-
128
-
129
-
130
-
131
-
132
-
133
-
134
-
135
-
136
-
137
-
138
-
139
-
140
-
141
-
142
-
143
-
144
-
145
-
146
-
147
-
148
-
149
-
150
-
151
-
152
-
153
-
154
-
155
-
156
-
157
-
158
-
159
-
160
-
161
-
162
-
163
-
164
-
165
-
166
-
167
-
168
 |
 |

offerings for members with complex chronic-care needs. The Metropolitan and SeniorBridge
acquisitions provide us with components of a successful integrated care delivery model that has
demonstrated scalability to new markets.
Other Businesses
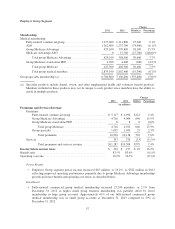
• As discussed in Note 17 to the consolidated financial statements included in Item 8. – Financial
Statements and Supplementary Data, future policy benefits payable include $1.4 billion at
December 31, 2013 associated with our non-strategic closed-block of long-term care insurance policies
acquired in connection with the 2007 acquisition of KMG. Approximately 33,300 policies remain in
force as of December 31, 2013. No new policies have been written since 2005 under this closed block.
During 2013, we recorded net benefits expense of $243 million ($154 million after-tax, or $0.99 per
diluted common share) for reserve strengthening related to this closed-block of long-term care
insurance policies.
• On June 26, 2013, the Puerto Rico Health Insurance Administration notified us of its election not to
renew our three-year Medicaid contracts for the East, Southeast, and Southwest regions which ended
June 30, 2013. Contractual transition provisions required the continuation of insurance coverage for
beneficiaries through September 30, 2013 and also require an additional period of time thereafter to
process residual claims.
• On January 27, 2014, we were notified by the Defense Health Agency of its intent to exercise its option
to extend our TRICARE South Region contract through March 31, 2015.
• Comparisons of the benefit ratios for the year ended December 31, 2013 and December 31, 2012
within Other Businesses are impacted by the transition to the current TRICARE South Region contract
on April 1, 2012, including a decrease in profitability under the current contract in connection with our
bid strategy, and the beneficial effect of a favorable settlement of contract claims with the Department
of Defense, or DoD, in the first quarter of 2013 primarily associated with previously disclosed
litigation settled in the second quarter of 2012.
Health Care Reform
The Patient Protection and Affordable Care Act and The Health Care and Education Reconciliation Act of
2010 (which we collectively refer to as the Health Care Reform Law) enacted significant reforms to various
aspects of the U.S. health insurance industry. While regulations and interpretive guidance on many provisions of
the Health Care Reform Law have been issued to date by the Department of Health and Human Services, or
HHS, the Department of Labor, the Treasury Department, and the National Association of Insurance
Commissioners, or NAIC, there are certain provisions of the law that will require additional guidance and
clarification in the form of regulations and interpretations in order to fully understand the impact of the law on
our overall business.
Implementation dates of the Health Care Reform Law began in September 2010 and continue through 2018,
and many aspects of the Health Care Reform Law are already effective and have been implemented by us.
Certain significant provisions of the Health Care Reform Law include, among others, mandated coverage
requirements, mandated benefits and guarantee issuance associated with commercial medical insurance, rebates
to policyholders based on minimum benefit ratios, adjustments to Medicare Advantage premiums, the
establishment of federally facilitated or state-based exchanges coupled with programs designed to spread risk
among insurers, an annual insurance industry premium-based assessment, and a three-year commercial
reinsurance fee. The following outlines certain provisions of the Health Care Reform Law:
•Currently Effective with Phased-In Implementation: In 2012, additional cuts to Medicare Advantage
plan payment benchmarks began to take effect (with plan payment benchmarks ultimately ranging from
95% in high-cost areas to 115% in low-cost areas of Medicare fee-for-service rates), with changes
49